


Irinotecan Hydrochloride concentrates for solution for infusion
Oct 25,2019
1. Name of the medicinal product
Irinotecan Hydrochloride medac 20 mg/ml, concentrate for solution for infusion.
2. Qualitative and quantitative composition
One millilitre of the concentrate for solution for infusion contains 20 mg irinotecan hydrochloride trihydrate, equivalent to 17.33 mg irinotecan.
Each vial of 2 ml contains 40 mg of irinotecan hydrochloride trihydrate (40 mg/2 ml).
Each vial of 5 ml contains 100 mg of irinotecan hydrochloride trihydrate (100 mg/5 ml).
Each vial of 15 ml contains 300 mg of irinotecan hydrochloride trihydrate (300 mg/15 ml).
Each vial of 25 ml contains 500 mg of irinotecan hydrochloride trihydrate (500 mg/25 ml).
Each vial of 50 ml contains 1000 mg of irinotecan hydrochloride trihydrate (1000 mg/50 ml).

3. Pharmaceutical form
Concentrate for solution for infusion.
A clear yellow solution.
pH 3.0 – 3.8
4. Clinical particulars
4.1 Therapeutic indications
Irinotecan Hydrochloride medac is indicated for the treatment of patients with advanced colorectal cancer
● as a single agent in patients who have failed an established 5-fluorouracil containing treatment regimen.
● in combination with 5-fluorouracil and folinic acid in patients without prior chemotherapy for advanced disease.
Irinotecan Hydrochloride medac in combination with cetuximab is indicated for the treatment of patients with epidermal growth factor receptor (EGFR)-expressing, KRAS wild-type metastatic colorectal cancer, who had not received prior treatment for metastatic disease or after failure of irinotecan-including cytotoxic therapy.
Irinotecan Hydrochloride medac in combination with 5-fluorouracil, folinic acid and bevacizumab is indicated for first-line treatment of patients with metastatic carcinoma of the colon or rectum.
Irinotecan Hydrochloride medac in combination with capecitabine with or without bevacizumab is indicated for first-line treatment of patients with metastatic colorectal carcinoma.
4.2 Posology and method of administration
The use of irinotecan should be confined to units specialised in the administration of cytotoxic chemotherapy and it should only be administered under the supervision of a physician qualified in the use of anticancer chemotherapy.
For posology and method of administration of concomitant cetuximab, refer to the product information for this medicinal product. Normally, the same dose of irinotecan is used as administered in the last cycles of the prior irinotecan-containing regimen. Irinotecan must not be administered earlier than 1 hour after the end of the cetuximab infusion.
Dose adjustments
Irinotecan should be administered after appropriate recovery of all adverse events to grade 0 or 1 NCI-CTC grading (National Cancer Institute Common Toxicity Criteria) and when treatment-related diarrhoea is fully resolved.
At the start of a subsequent infusion of therapy, the dose of irinotecan, and 5-FU when applicable, should be decreased according to the worst grade of adverse events observed in the prior infusion. Treatment should be delayed by 1 – 2 weeks to allow recovery from treatment-related adverse events.
With the following adverse events a dose reduction of 15 – 20 % should be applied for irinotecan and/or 5-FU when applicable:
● Haematological toxicity (neutropenia grade 4, febrile neutropenia [neutropenia grade 3 – 4 and fever grade 2 – 4], thrombocytopenia and leukocytopenia).
● Non-haematological toxicity.
Recommendations for dose modifications of cetuximab when administered in combination with irinotecan must be followed according to the product information for this medicinal product.
Refer to the bevacizumab summary of product characteristics for dose modifications of bevacizumab when administered in combination with irinotecan/5-FU/FA.
In combination with capecitabine for patients 65 years of age or more, a reduction of the starting dose of capecitabine to 800 mg/m2 twice daily is recommended according to the summary of product characteristics for capecitabine. Refer also to the recommendations for dose modifications in combination regimen given in the summary of product characteristics for capecitabine.
Treatment duration
Treatment with irinotecan should be continued until there is an objective progression of the disease or an unacceptable toxicity.
Special populations
Patients with impaired hepatic function
In monotherapy:
Blood bilirubin levels (up to 3 times the upper limit of the normal range [ULN]) in patients with WHO performance status ≤ 2 should determine the starting dose of irinotecan. In these patients with hyperbilirubinaemia and prothrombin time greater than 50 %, the clearance of irinotecan is decreased and therefore the risk of haematotoxicity is increased. Thus, weekly monitoring of complete blood counts should be conducted in this patient population.
In patients who experienced severe haematological events, a dose reduction is recommended for subsequent administration.
There is an increased risk of infections and haematological toxicity in patients with severe diarrhoea. In patients with severe diarrhoea, complete blood cell counts should be performed.
Liver impairment
Liver function tests should be performed at baseline and before each cycle.
Weekly monitoring of complete blood counts should be conducted in patients with bilirubin ranging from 1.5 to 3 times the ULN, due to decrease of the clearance of irinotecanand thus increasing the risk of haematotoxicity in this population.
Nausea and vomiting
A prophylactic treatment with antiemetics is recommended before each treatment with irinotecan. Nausea and vomiting have been frequently reported. Patients with vomiting associated with delayed diarrhoea should be hospitalised as soon as possible for treatment.
Acute cholinergic syndrome
If acute cholinergic syndrome appears (defined as early diarrhoea and various other signs and symptoms such as sweating, abdominal cramping, myosis and salivation), atropine sulphate (0.25 mg subcutaneously) should be administered unless clinically contraindicated.
These symptoms may be observed during or shortly after infusion of irinotecan, are thought to be related to the anticholinesterase activity of the irinotecan parent compound, and are expected to occur more frequently with higher irinotecan doses.
Caution should be exercised in patients with asthma. In patients who experienced an acute and severe cholinergic syndrome, the use of prophylactic atropine sulphate is recommended with subsequent doses of irinotecan.
Respiratory disorders
Interstitial pulmonary disease presenting as pulmonary infiltrates is uncommon during irinotecan therapy. Interstitial pulmonary disease can be fatal. Risk factors possibly associated with the development of interstitial pulmonary disease include the use of pneumotoxic medicinal products, radiation therapy and colony stimulating factors. Patients with risk factors should be closely monitored for respiratory symptoms before and during irinotecan therapy.
Extravasation
While irinotecan is not a known vesicant, care should be taken to avoid extravasation and the infusion site should be monitored for signs of inflammation. Should extravasation occur, flushing the site and application of ice is recommended.
Elderly
Due to the greater frequency of decreased biological functions, in particular hepatic function, in elderly patients, dose selection with irinotecan should be cautious in this population.
Patients with chronic inflammatory bowel disease and/or bowel obstruction
Patients must not be treated with irinotecan until resolution of the bowel obstruction.
Patients with impaired renal function
Increases in serum creatinine or blood urea nitrogen have been observed. There have been cases of acute renal failure. These events have generally been attributed to complications of infection or to dehydration related to nausea, vomiting, or diarrhoea. Rare instances of renal dysfunction due to tumour lysis syndrome have also been reported.
Further, studies in this population have not been conducted .
- Related articles
- Related Qustion
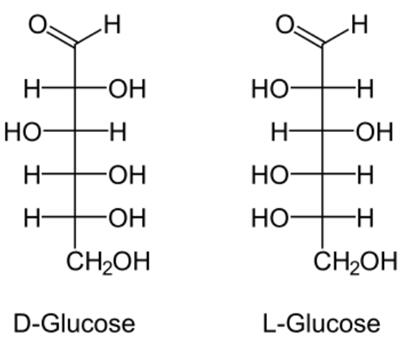
L-Glucose naturally occurs in fruits and other parts of plants in its free state. However, it is not present in higher living organisms.....
Oct 25,2019Saccharides
Olive oil is used to prevent heart attack and stroke (cardiovascular disease), breast cancer, colorectal cancer, ovarian cancer, rheumatoid arthritis, and migraine headache.....
Oct 25,2019Plant extracts
Irinotecan hydrochloride
100286-90-6You may like
- Diosgenin:Uses,Functions and Synthesis
Dec 12, 2025
- Biosynthesis of Cyclopamine from Cholesterol
Dec 10, 2025
- Synthesis of ribociclib
Dec 10, 2025
Irinotecan hydrochloride manufacturers
- Irinotecan hydrochloride
-

- $1.00 / 1KG
- 2025-12-13
- CAS:100286-90-6
- Min. Order: 1KG
- Purity: 98.0 ~ 102.0%
- Supply Ability: 1ton/month
- Irinotecan hydrochloride
-

- $0.00 / 1KG
- 2025-12-13
- CAS:100286-90-6
- Min. Order: 1KG
- Purity: ≥98% HPLC
- Supply Ability: 1000KG
- Irinotecan hydrochloride
-

- $5.00/ KG
- 2025-12-12
- CAS:100286-90-6
- Min. Order: 1KG
- Purity: 99% hplc
- Supply Ability: 500TONS