


How can Epinephrine be used as a Vasoconstrictor?
Sep 18,2020
Epinephrine is a naturally occurring catecholamine secreted by the adrenal medulla, consisting of approximately 80% of its secretions. It is also available as a synthetic catecholamine, which is identical in structure with the natural hormone epinephrine. Epinephrine is the most widely used vasoconstrictor in dentistry and the most potent. Epinephrine is the standard by which all other vasoconstrictors are measured (Table 1).
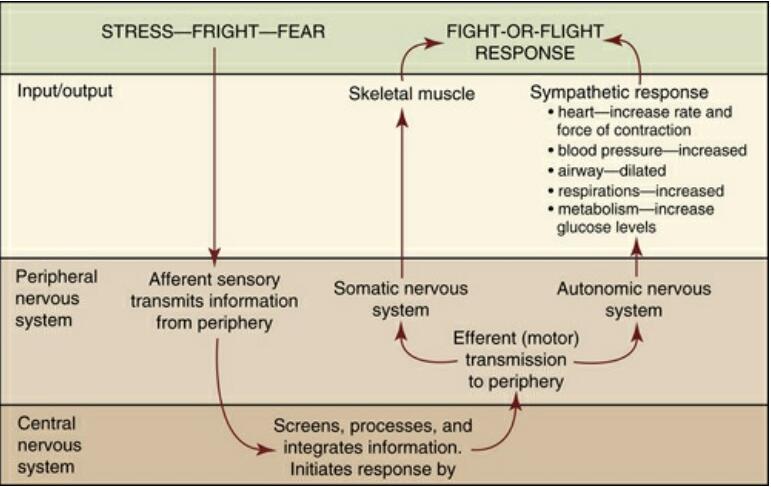
FIGURE 1 Nervous system response during “fight-or-flight” or stress. (From McKenry L, Tessier E, Hogan M: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
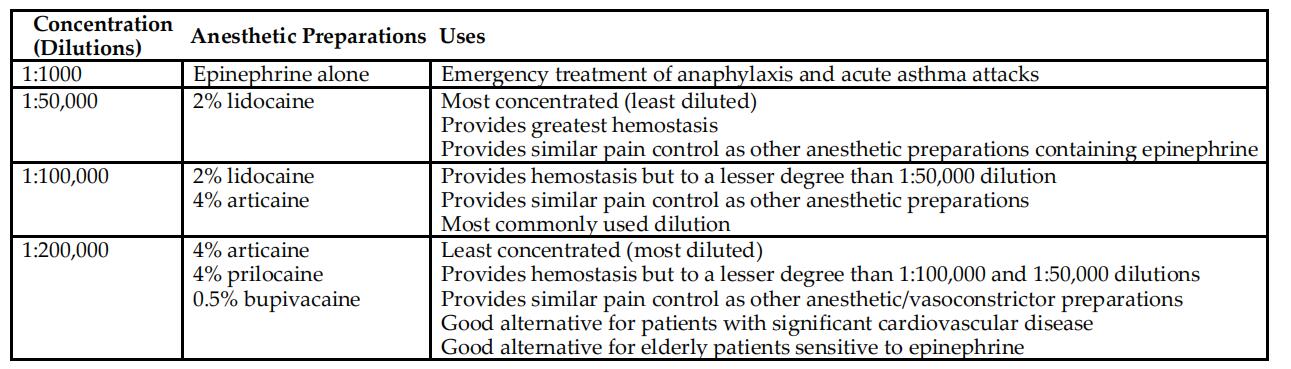
TABLE 1
Epinephrine (Adrenalin) Dilutions and Uses in Dentistry
Mechanism of Action
Epinephrine and norepinephrine cause vasoconstriction by activating adrenergic receptors located in most tissues. According to Ahlquist2 in 1948, these targeted receptor sites are divided into two major groups of adrenergic receptors, alpha (α) and beta (β), with several subtypes. Ahlquist recognized that α receptors have excitatory actions, and β receptors have inhibitory actions from catecholamines on smooth muscles. The excitatory action of α receptors by sympathomimetic drugs causes vasoconstriction of the smooth muscle in blood vessels. These α receptors have been further subcategorized into α1 and α2 depending upon differences in their location and function, α1 receptors are excitatory-postsynaptic and α2 receptors are inhibitory-postsynaptic.1,2 The inhibitory action of β receptors by sympathomimetic drugs causes smooth muscle relaxation (vasodilation and bronchodilation), and cardiac stimulation. The β receptors have also been further subcategorized into β1 found in the heart (causing cardiac stimulation) and small intestines (causing lipolysis), and β2 found in the bronchi, vascular beds, and uterus causing bronchodilation and vasodilation.
Norepinephrine activates predominantly α receptors, and epinephrine activates both α and β receptors, causing vasoconstriction and vasodilation respectively. α Receptors are less sensitive to epinephrine.3 However, once the α receptor is stimulated by high levels of epinephrine, this activation will override the vasodilation caused by β receptors and subsequently will cause vasoconstriction of the smooth muscle in peripheral arterioles and veins. This is the main reason sympathomimetic agents are added to local anesthetic solutions.
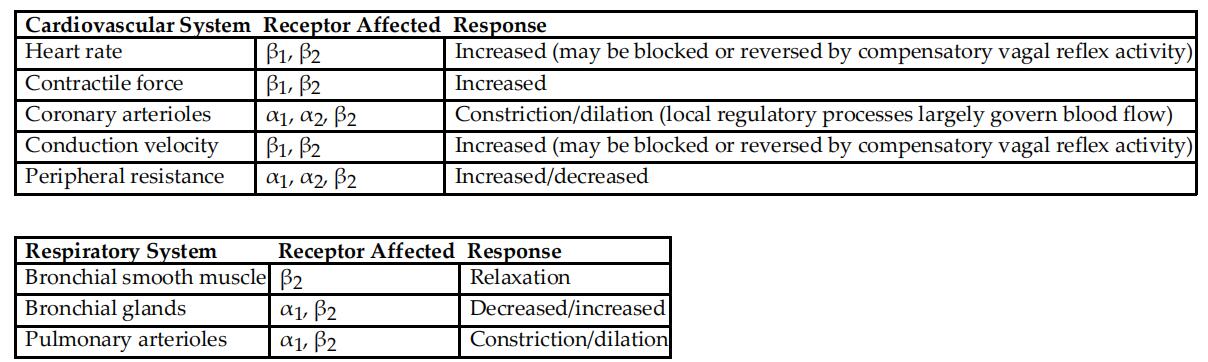
Stimulation of α receptors by adrenergic drugs such as epinephrine causes constriction of the smooth muscle in the blood vessels, also referred to as vasoconstriction. β2 Receptor activation by epinephrine relaxes bronchial smooth muscles, causing the bronchi of the lungs to dilate. In addition, β1 receptors have stimulatory effects that increase the rate and force of heart contractions. These stimulatory effects on β1 receptors are undesirable side effects of incorporating sympathomimetic agents such as epinephrine into local anesthetic solutions. This is of particular concern in patients with preexisting cardiovascular and thyroid disease. The risks of adding the vasoconstrictor to the local anesthetic must be weighed against the benefits, and decreasing the amount of the drug administered should be considered (discussed next). Table 4-2 lists the major systemic effects of injected sympathomimetic agents involved in the cardiovascular and respiratory systems.
Epinephrine Dilutions
The concentration of vasoconstrictors in local anesthetic solutions is referred to as a ratio rather than a percentage as expressed by the local anesthetic drug. For example, a concentration of 1:100,000 means there is 1 g (or 1000 mg) of drug contained (dissolved) in a 100,000 mL solution, or 0.01 mg/mL. The most common dilutions of epinephrine combined with local anesthetics are 1:50,000 (0.02 mg/mL), 1:100,000 (0.01 mg/mL), and 1:200,000 (0.005 mg/mL). The 1:50,000 dilution is manufactured in combination with 2% lidocaine, the 1:100,000 dilution is manufactured in combination with 2% lidocaine and 4% articaine, and the 1:200,000 dilution is manufactured in combination with 4% prilocaine, 4% articaine, and 0.5% bupivacaine. Therefore, in a typical dental anesthetic cartridge containing both a local anesthetic drug and vasoconstrictor, the label will identify both drugs. Using prilocaine with epinephrine as an example, the cartridge may contain 4% prilocaine (referred to as a percentage) with 1:200,000 epinephrine (referred to as a ratio) . Table 2 lists the vasoconstrictor dilutions combined with dental local anesthetics used in the United States and Canada.
TABLE 2
Systemic Effects of Adrenergic Amines on the Cardiovascular and Respiratory Systems
The 1:50,000 dilution represents the highest concentration, and 1:200,000 dilution represents the lowest concentration and therefore produces fewer side effects.1 Concentrations greater than 1:200,000 offer no advantage in prolonging the duration of anesthesia, reducing the plasma levels, or advancing pain control. Therefore, because a 1:50,000 offers no added benefits to most clinical situations and can produce more profound undesired sympathomimetic actions (fight or flight), there is questionable rationale for using a 1:50,000 dilution of epinephrine for pain control. However, higher concentrations of epinephrine, specifically the 1:50,000 dilution are more effective for bleeding control (hemostasis). Local anesthetics with vasoconstrictors may be infiltrated for hemostasis even when pulpal anesthesia has been obtained. Therefore, using a 1:100,000 dilution of epinephrine for obtaining pulpal anesthesia may be used in combination with a relatively small infiltrated dose of 1:50,000 dilution of epinephrine into the papilla or gingival margin to decrease bleeding to less than half of that recorded from a similar volume of 1:100,000. This is particularly important for bleeding control during periodontal surgeries and for dental hygienists providing nonsurgical periodontal therapy.
- Related articles
- Related Qustion
- The Pharmacodynamics of L(-)-Epinephrine and Its Role in Anaphylaxis Management Dec 26, 2023
L(-)-Epinephrine is a sympathomimetic drug that activates beta-1 and beta-2 receptors, providing relief from asthma, croup, anaphylaxis, and allergic reactions, with rapid metabolism and elimination.
- L(-)-Epinephrine: Physiological effects and clinical applications Aug 2, 2023
L(-)-Epinephrine regulates blood pressure, heart rate, metabolism, and the immune system. It is used in resuscitation and anesthesia.
- Uses of Epinephrine Dec 22, 2021
Epinephrine stimulates both the alpha- and beta-adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels. It is also used as a vasoconstrictor, car

Olmesartan medoxomil is a white to light yellowish-white powder or crystalline powder with a molecular weight of 558.59. It is practically insoluble in water and sparingly soluble in methanol.....
Sep 18,2020API
Lidocaine was the first amide local anesthetic suitable for nerve blocks in dentistry and because of its reliability is currently the most commonly used local anesthetic solution in dentistry in the United States.....
Sep 18,2020API
L(-)-Epinephrine
51-43-4You may like
L(-)-Epinephrine manufacturers
- L(-)-Epinephrine
-

- $1905.00 / 1KG
- 2025-12-03
- CAS:51-43-4
- Min. Order: 1KG
- Purity: 99%
- Supply Ability: 10000kg
- L(-)-Epinephrine
-

- $0.00 / 1kg
- 2025-06-20
- CAS:51-43-4
- Min. Order: 1kg
- Purity: 0.99
- Supply Ability: 20tons
- L(-)-Epinephrine
-
- $100.00 / 1KG
- 2025-06-03
- CAS:51-43-4
- Min. Order: 10KG
- Purity: 0.99
- Supply Ability: 20tons